
Epinephrine Auto-Injector Technique Checker
Check if you're using the correct technique for epinephrine administration. Based on CDC and school safety guidelines.
When a child goes into anaphylaxis, every second counts. A delay of even one minute can mean the difference between life and death. Yet, in schools across the U.S., trained staff still hesitate - not because they don’t care, but because they’re unsure. Was that a mild rash or the start of something worse? Did they hold the injector long enough? Was it aimed at the right spot? These aren’t hypothetical questions. They’re real, life-or-death moments that happen every day.
Why Timing Is Everything
Studies show that 95% of anaphylaxis deaths happen within 48 hours of the first symptom, but most occur within the first five minutes. The epinephrine auto-injector is the only treatment that can stop this process. It doesn’t just ease symptoms - it reverses the body’s deadly response. But if it’s not given quickly, or if it’s given wrong, it doesn’t work. And here’s the scary part: in nearly 83% of fatal cases, epinephrine was never administered at all. Why? Because people mistook the signs.
It’s not always a swollen throat or trouble breathing. Sometimes, it’s just a sudden flush of the face, a strange feeling of warmth, or a child suddenly saying they feel "weird." These are early warning signs. Training that only teaches the "classic" symptoms misses half the cases. Effective training teaches you to trust the whole picture - not just one symptom.
Where You Inject Matters More Than You Think
It’s not enough to know how to press the device. You have to know where to press it. The only correct injection site is the lateral thigh - the outer side, halfway between the hip and knee. Injecting into the front of the thigh, the buttocks, or even through thick clothing can mean the medicine doesn’t absorb fast enough - or at all.
California’s 2023 training standards make this crystal clear: the injection must go into bare skin. A teacher once tried to inject through jeans during a drill. The device clicked, but the needle never reached the muscle. No epinephrine got into the bloodstream. That’s not a rare mistake. Research from the University of Michigan found that 29% of untrained people inject in the wrong spot. And here’s the kicker: most auto-injectors don’t have visual guides on the device itself. You have to know it by heart.
Device Differences Can Kill
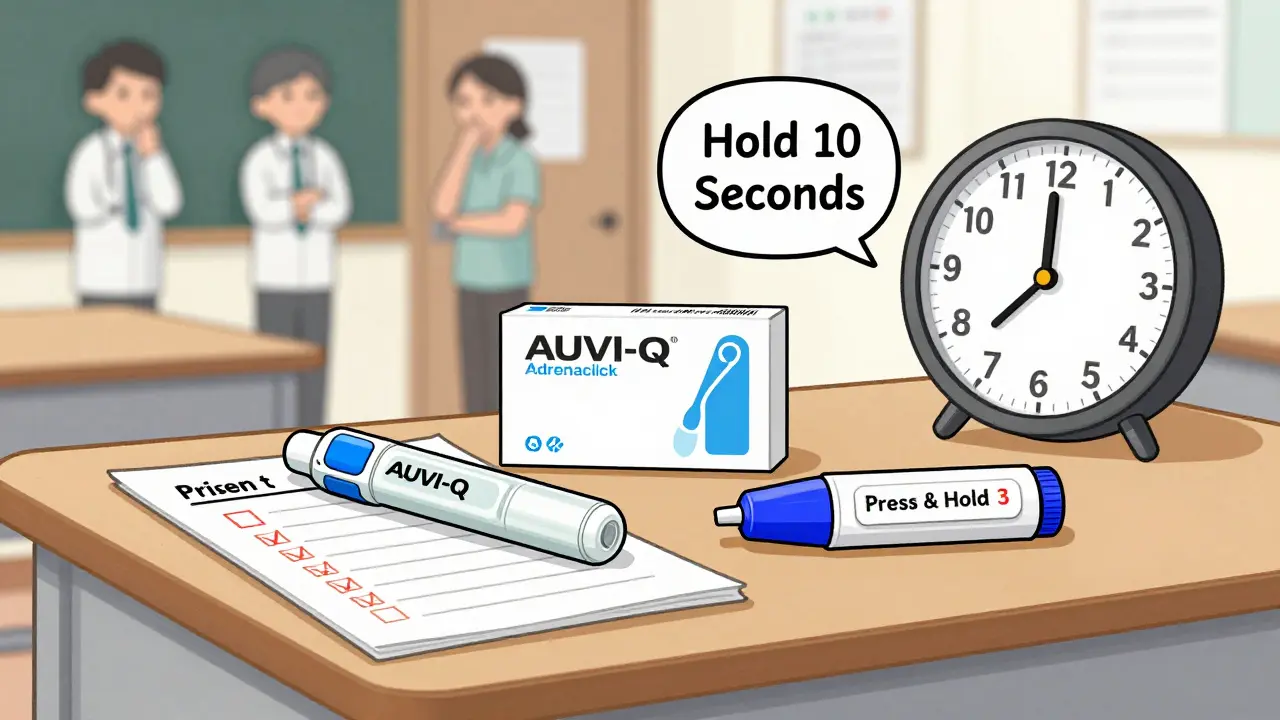
Not all auto-injectors are the same. EpiPen, AUVI-Q, and Adrenaclick all work differently. If you train on one, you might fumble with another. AUVI-Q, for example, gives voice prompts and requires you to hold it for 10 seconds. EpiPen doesn’t talk - you just press and hold for 3 seconds. If you’re used to one and handed another in a real emergency, you might stop too soon.
That’s why hands-on practice with the actual device used in your school is non-negotiable. A 2022 study in the Journal of School Nursing found that training with real devices (not just trainers) cut administration errors by 78%. And it’s not just about muscle memory - it’s about confidence. People who’ve held the real thing, felt the click, and heard the warning sound don’t freeze. They act.
Two Injectors Are Not Optional
One auto-injector is never enough. Up to 35% of anaphylaxis cases need a second dose. And it’s not because the first one failed - it’s because the reaction can come back. This is called a biphasic reaction. It can happen hours later, even if the person seemed fine after the first shot.
Food Allergy Research & Education (FARE) says every school should have two injectors on hand - one for immediate use, one as backup. But in 40% of schools, only one is kept in the nurse’s office. The other is stored in a locked cabinet, in a different building, or with a staff member who’s out on lunch duty. That’s not a policy gap - that’s a death sentence waiting to happen.
Training That Doesn’t Stick Is Dangerous
Most schools do a one-time training session in September. Then they forget about it until next year. That’s a disaster. Skill retention drops to 47% after just six months without practice. That means half the people trained in September won’t remember how to use the device by March.
The National Association of School Nurses found that only 22% of districts require annual refresher training. That’s not enough. You wouldn’t let someone drive a car after one lesson and never practice again. Why treat a life-saving device any differently?
The best programs don’t just do a lecture. They run drills. Quarterly. With expired injectors. With real-time feedback. In Texas, one district started doing 10-minute refreshers every three months. They had two real anaphylaxis events last year. Both were handled perfectly. No hesitation. No mistakes.
Legal Fear Is Real - And It’s Wrong
One of the biggest reasons staff hesitate? Fear of getting sued. But here’s the truth: every state has a Good Samaritan law that protects anyone who acts in good faith to help someone in an emergency. You can’t be held liable for trying to save a life. In fact, failing to act can put the school at greater legal risk.
A 2022 survey of over 2,000 school nurses found that 42% of staff said they feared legal consequences. That’s not a training problem - it’s a communication problem. Schools need to give staff a signed document that says: "You are protected by law if you use the auto-injector in good faith." Put it in their employee handbook. Say it at every meeting. Repeat it until it’s common knowledge.
What Great Training Looks Like
Effective training isn’t a PowerPoint. It’s a living system. Here’s what works:
- Hands-on practice with the exact device used in your school - every year
- Drills that simulate real symptoms - not just textbook cases
- Clear rules on when to give a second dose (at least 5 minutes after the first, if symptoms return)
- Training that includes how to monitor the person after injection - check breathing, heart rate, skin color
- Keeping two injectors accessible at all times - not locked away
- Using video training (like OhioTRAIN) to reinforce steps visually
California’s standards require written materials to be kept for three years. That’s not just bureaucracy - it’s accountability. If a student has a reaction next year, you need to prove you trained the staff. And if you didn’t? You’re liable.
What’s Changing in 2026
Virtual reality training is no longer science fiction. The American Red Cross launched a VR module in April 2023 that cuts training time by 35% and improves long-term retention by 28%. Staff put on a headset, face a simulated child having a reaction, and practice in a safe, repeatable environment. They learn to recognize subtle signs, handle device confusion, and stay calm under pressure.
Ohio schools are already syncing training records with their health databases. If someone’s training expires, the system flags it. If an injector is out of date, it alerts the nurse. This isn’t futuristic - it’s necessary. And it’s coming to more districts in 2026.
Don’t Wait for a Crisis
Anaphylaxis doesn’t announce itself. It doesn’t happen during school hours. It doesn’t care if you’re busy or tired or unsure. It just happens. And if you’re not ready, someone could die - not because they were allergic, but because the people around them didn’t know what to do.
Training isn’t about compliance. It’s about courage. It’s about knowing, without a doubt, that you can act - and that you’ll act fast. Because when seconds matter, confidence isn’t optional. It’s everything.

Comments
Chris Crosson
Had a kid go into anaphylaxis last year during gym class. We had the EpiPen, but the teacher panicked and injected through his hoodie. No effect. Kid was fine because EMS got there in 4 minutes, but that was pure luck. This post? 100% spot on. We’re doing drills now. Quarterly. With expired pens. It’s wild how much difference it makes when you’ve actually felt the click.
Also, the voice-prompt AUVI-Q? Game changer. No confusion. No second-guessing. If your school still uses EpiPens, start pushing for the upgrade. It’s not about brand loyalty-it’s about survival.
Linda Foster
While the intent of this article is commendable, I must emphasize the importance of adhering strictly to institutional protocols regarding medical device administration. Unauthorized or improvised training methodologies may inadvertently compromise established safety frameworks. Furthermore, the legal implications of non-standardized procedures warrant careful review by district legal counsel prior to implementation.
Darlene Gomez
I’ve been a school nurse for 18 years. I’ve seen kids turn blue. I’ve held their hands while they gasped. And I’ve watched teachers freeze-not because they’re uncaring, but because they’ve been trained like robots, not humans.
The real issue isn’t the device. It’s the fear. The fear of doing it wrong. The fear of being blamed. The fear that someone else should’ve done it better.
What works? Repetition. Realism. Role-playing. Not PowerPoint slides. Not a one-hour seminar in September. I run mock emergencies every quarter. Kids fake-seizure. Teachers scream. Someone yells "IT’S PEANUT BUTTER!" And then-boom-we do the injection. Bare skin. Thigh. 3 seconds. We debrief. We laugh. We cry. And then? They remember.
You don’t train for emergencies. You train for humanity. And humanity doesn’t work on schedules. It works on trust.
Katie Putbrese
Why are we letting the government tell us how to save lives? This whole system is a bureaucratic nightmare. Why can’t we just let parents handle it? My kid’s got an EpiPen. I carry it. I train the teachers. Why does the school need two? Why does it need drills? Why does it need VR? This is socialism disguised as safety.
And don’t get me started on the "Good Samaritan" lie. Lawyers are waiting to pounce. You think you’re protected? You’re just a target with a clipboard.
Stop the training. Stop the drills. Stop the fear-mongering. Let parents do what they’re supposed to do-raise their own kids.
Amber Gray
lmao so now we need vr and 2 epipens and drills?? bro its a peanut allergy not a nuclear war. just give the kid a benadryl and call 911. stop overcomplicating everything. #epipenoverkill #freeourkids
James Moreau
As someone who works with international school systems, I’ve seen how this plays out differently overseas. In Japan, for example, they use a single standardized device with tactile feedback. No voice prompts. No confusion. Just one tool, one method, one clear protocol.
Maybe we’re over-engineering this. The goal isn’t to make training flashy-it’s to make it universal. Simplicity saves lives.
J. Murphy
epinephrine is just a stimulant. you dont need it. the body can handle it. this whole thing is a scam by big pharma. they sell you the pens and then make you pay for training. next theyll sell you vr headsets for sneezing. lol
Jesse Hall
Y’all. I work in a rural school. We had a kid go into anaphylaxis last month. We used the EpiPen. We did the drill. We held it. We didn’t panic. We didn’t overthink. We just acted.
And you know what? He’s back in class. Laughing. Eating apple slices. No big deal.
But it could’ve been. So yeah-do the drills. Keep two pens. Train like your life depends on it. Because it does. 💪❤️
Donna Fogelsong
Did you know the CDC is secretly tracking all epinephrine usage through implanted microchips? The "biphasic reaction" is a manufactured statistic to justify funding. The real reason schools need two injectors? So they can monitor your child’s immune response in real time. The 2026 VR training? It’s not for learning. It’s for data harvesting. Wake up. This isn’t health. It’s control.
rebecca klady
My son’s allergic to cashews. We had a scare last year. The nurse didn’t know how to use the AUVI-Q. She used the EpiPen trainer. Said she’d "never seen the real thing." I cried. Then I bought two real ones and left them in the office with a note: "If he turns red, just press. Don’t think. Just press." I don’t care about drills. I care about someone not freezing.
Namrata Goyal
in usa you overreact to everything. in india we just give antihistamine and move on. why you need 2 epipen? why vr? why drills? your system is broken. this is not science. this is fear industry. you make money from panic. simple solution: dont let allergic kids go to school. problem solved.