When your doctor suspects a heart problem, two tests often come up: cardiac MRI and echocardiography. Both show your heart in detail, but they’re not the same. One uses sound waves. The other uses magnets. One is fast and available in most clinics. The other is slower, more expensive, but gives a level of detail you can’t get anywhere else. So which one do you actually need?
What Echocardiography Can and Can’t Do
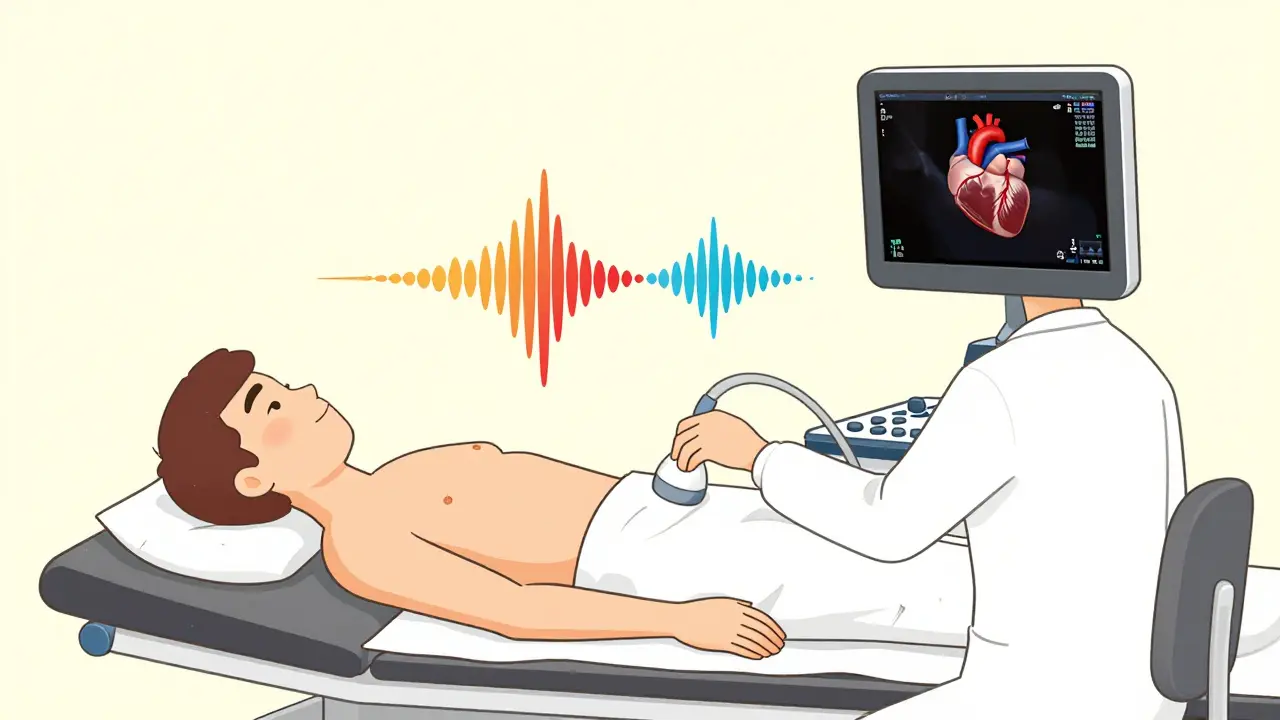
Echocardiography, or echo, has been the go-to heart test for over 70 years. It’s the ultrasound of the heart. A technician moves a small device across your chest. It sends out high-frequency sound waves that bounce off your heart and create moving images on a screen. You can see your heart beating in real time - valves opening and closing, walls thickening or thinning, blood flowing through chambers.
It’s cheap. Most places charge between $500 and $1,500. It’s quick - usually under 30 minutes. And it’s everywhere. Even small hospitals and emergency rooms have an echo machine. That’s why over 15 million echocardiograms are done in the U.S. every year.
Normal echo numbers? Left ventricle size between 37-56 mm. Wall thickness 6-11 mm. Ejection fraction (EF) - how well your heart pumps - should be 50-75%. But here’s the catch: echo makes assumptions. It guesses the shape of your heart to calculate volume. If your heart isn’t a perfect oval (and most aren’t), those numbers can be off. A 2023 study in the American Journal of Cardiology found echo measurements were consistently 19% higher than cardiac MRI for wall thickness. That’s not a small error - it can mean misdiagnosing thickening or missing early disease.
Another issue? Acoustic windows. If you’re overweight, have lung disease, or your ribs block the view, the images get blurry. I’ve seen cases where a patient had a normal echo but still felt terrible. Their heart was actually failing - the echo just couldn’t see it clearly. That’s when MRI steps in.
Why Cardiac MRI Is the Gold Standard
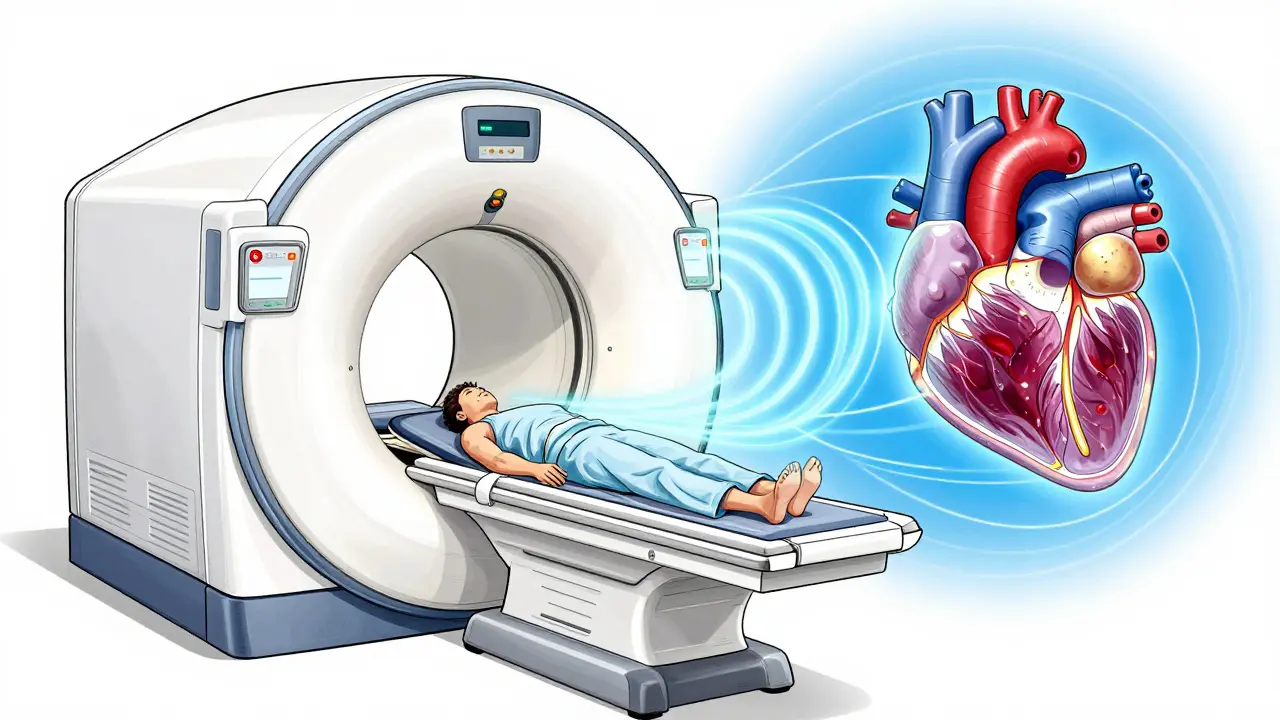
Cardiac MRI doesn’t use sound. It uses a powerful magnet - usually 1.5 to 3 Tesla - along with radio waves to build a 3D picture of your heart. No guessing. No assumptions. It counts every pixel. It measures volume directly, slice by slice. That’s why it’s called the reference standard.
Normal MRI numbers? Left ventricular volume: 67-155 mL for men, 55-105 mL for women. Mass: 49-115 g for men, 37-81 g for women. These numbers are more accurate because MRI doesn’t rely on geometry. It sees the whole thing.
But MRI’s real superpower is tissue. It can spot scar tissue, inflammation, and early fibrosis - things echo can’t touch. Late gadolinium enhancement (LGE) shows where heart muscle has been damaged. In conditions like myocarditis or sarcoidosis, echo might look normal. MRI shows the inflammation before your heart even starts to weaken.
A 2023 study in JACC: CardioOncology found that 2D echo underestimated ejection fraction by 3% on average - and sometimes by as much as 15%. That’s critical for cancer patients. If you’re on chemo that’s hard on the heart, you need to know if your EF is dropping. Echo missed it in 10% of cases. MRI caught it.
Reproducibility? MRI wins again. Inter-observer variability (how much different doctors agree on measurements) is 2.6% for MRI. For echo, it’s 6.8%. That means two cardiologists might give you different EF numbers on echo. On MRI? They’ll likely say the same thing.
When Echo Falls Short - And MRI Saves the Day
Here’s where the real-world difference matters.
One patient I read about had chest pain and shortness of breath. Echo showed normal EF - 60%. But she was exhausted. A cardiac MRI revealed patchy scarring in her heart muscle. She had early myocarditis. She started treatment. Six months later, her symptoms were gone.
Another case: a 52-year-old man with a family history of sudden cardiac death. Echo showed normal walls. MRI showed a thickened septum with fibrosis - classic hypertrophic cardiomyopathy. Without MRI, he’d have been told he was fine. He got an ICD implanted. He’s alive today.
Surveys show 76% of cardiologists use MRI when echo is inconclusive. In academic centers, MRI is standard for diagnosing myocarditis (used in 85% of cases), cardiac sarcoidosis (92%), and before ablation for arrhythmias (76%).
But MRI isn’t perfect. It’s slow. A full scan takes 45-60 minutes. You have to lie still. If you have an irregular heartbeat, it gets harder. Some patients panic in the tube. And if you have a pacemaker, defibrillator, or certain metal implants, you might not be able to have one at all.
Cost, Access, and the Real-World Gap
Cardiac MRI costs $1,500 to $3,500. Echo? Half that. In community hospitals, 78% have echo available the same day. Only 35% offer MRI within a week. Wait times for non-urgent MRI? Often over 14 days. A 2023 survey found 68% of cardiologists in the U.S. had to wait longer than two weeks for a patient’s scan.
That’s why echo still rules. It’s the first step. The screening tool. The emergency tool. If you’re in the ER with chest pain, you get echo. If you’re stable and your echo is unclear? Then MRI.
Technology is closing the gap. New 3D echo systems now match MRI for EF accuracy in many cases. Philips’ EPIQ CVx uses AI to auto-calculate volumes, cutting variability to 4.2%. Siemens introduced a 0.55T MRI in 2023 - low enough to safely scan patients with older pacemakers. That’s a game-changer.
But even with these advances, MRI still leads in tissue detail. No echo system can show fibrosis like LGE. No echo can quantify myocardial strain with the same precision as MRI’s tagging sequences.
What Your Doctor Really Thinks
Dr. Raymond Kwong from Brigham and Women’s says MRI’s low variability makes it superior for tracking heart function over time. If you’re on a drug that affects your heart - like chemo or certain blood pressure meds - you want MRI for follow-ups.
Dr. Susan Joseph from Johns Hopkins puts it bluntly: “Echo tells you the heart is working. MRI tells you why it’s working - or why it’s not.”
But Dr. Michael Chen from the American Society of Echocardiography reminds us: “3D echo has closed the gap. If you have access to it, use it first.”
The truth? It’s not an either/or. It’s a sequence. Echo first. MRI if needed.
Which Test Should You Get?
Here’s a simple guide:
- Get echocardiography if: You’re having symptoms like shortness of breath, fatigue, or palpitations for the first time. You’re being checked after a heart attack. You’re monitoring known valve disease. You’re in an emergency.
- Get cardiac MRI if: Echo was inconclusive. You have unexplained heart failure. You’re being evaluated for myocarditis, sarcoidosis, or inherited cardiomyopathy. You’re on heart-toxic chemotherapy. You’ve had a sudden cardiac arrest with no clear cause. You need precise measurements for surgery or transplant evaluation.
Bottom line: Echo is your starting point. MRI is your deep dive. One isn’t better - they’re complementary. The best care uses both when needed.
What’s Coming Next
By 2030, experts predict hybrid protocols will be standard. Imagine: You get a quick echo in the clinic. It shows something odd. You go to MRI the next day for tissue mapping. The two images are fused. Your doctor sees both structure and scar in one view.
Parametric mapping - measuring T1, T2, and ECV - is already here. It quantifies tissue changes before symptoms appear. In early-stage amyloidosis, MRI can detect protein buildup in the heart wall years before echo shows thickening.
AI is helping both. Automated echo analysis cuts human error. AI-driven MRI reconstruction cuts scan time. The future isn’t choosing one over the other. It’s using them together.

Comments
Robert Shiu
Man, I love how this post breaks it down. I work in a rural ER and we do echo every day-sometimes 5-6 a shift. But I’ve seen patients come in with normal echoes and still be in full-blown heart failure. One guy had a 65% EF on echo, but his MRI showed 38% and massive fibrosis. We almost missed it. Cardiac MRI isn’t perfect, but when echo says ‘fine’ and the patient looks like they’re dying? Trust the magnet.
Also, shoutout to AI-enhanced echo. We just got a new machine with auto-vol tracking. It’s not MRI-level, but it’s cut our inter-observer variability in half. Still, if I’m tracking chemo patients? I’m pushing for MRI. No debate.
Caleb Sciannella
It is of considerable importance to acknowledge the methodological rigor that underpins cardiac magnetic resonance imaging as the current reference standard for volumetric and tissue characterization in cardiovascular pathology. The precision afforded by slice-by-slice quantification, coupled with the absence of geometric assumptions inherent in two-dimensional echocardiographic models, renders MRI indispensable in clinical decision-making for complex cardiomyopathies.
Moreover, the reproducibility metrics cited-namely, a 2.6% inter-observer variability for MRI versus 6.8% for echo-are statistically significant and clinically meaningful, particularly in longitudinal monitoring scenarios such as oncology-induced cardiotoxicity. While echo remains a pragmatic first-line modality due to its accessibility and cost-effectiveness, it is my professional opinion that MRI should be elevated to a tier-one diagnostic tool in all cases where diagnostic ambiguity persists.
Davis teo
Okay, but have you ever been in an MRI tube for 50 minutes while your heart is racing and you’re sweating bullets because you’re claustrophobic? I have. I had a weird rhythm, got echo first-looked fine. Then they made me do MRI. I screamed. The tech had to stop. I cried. I apologized. I still got the scan the next day with a sedative.
Meanwhile, my cousin got a 3D echo and they caught her LGE scar in 12 minutes. No tube. No panic. Just a tech saying, ‘Hey, you’ve got some scarring.’
So yeah, MRI’s fancy. But sometimes, the machine that doesn’t make you want to jump out a window is the one that saves your life. Just saying.
Michaela Jorstad
Yes. Yes. Yes. I’ve been a cardiac nurse for 18 years. I’ve seen too many patients dismissed because their echo was ‘normal.’ One woman came in with fatigue, dizziness, chest pressure-echo said ‘mild LVH.’ MRI showed massive fibrosis from undiagnosed sarcoidosis. She was 32. Had no family history. No symptoms before. Just… tired.
And then there’s the cost issue. Insurance denies MRI unless you have ‘clear indication.’ But what if echo is borderline? What if your EF is 48%? Is that ‘clear’? No. It’s gray. And gray is where people slip through.
Please, doctors: If echo is ‘inconclusive,’ don’t wait. Push for MRI. It’s not ‘overkill.’ It’s justice.
Chris Beeley
As a cardiology fellow trained in Lagos and now working in Boston, I find it amusing how Western medicine fetishizes MRI as some kind of divine oracle. In Nigeria, we use echo because it’s all we have-and we’re damn good at it. We don’t have 3T scanners, but we have trained eyes, experienced hands, and a deep understanding of clinical context.
Do you know how many patients in the U.S. get unnecessary MRIs because they’re scared of ‘missing something’? Meanwhile, in Africa, we diagnose hypertrophic cardiomyopathy with a stethoscope, echo, and a patient’s story. And we’re right 90% of the time.
Stop treating technology as a substitute for clinical wisdom. Echo isn’t ‘flawed’-it’s contextual. MRI is expensive. Echo is human. And sometimes, human judgment beats a 3T magnet.
Amrit N
i read this whole thing and honestly i think echo is good enough for most people. like yeah mrI is fancy and all but my uncle got his echo and they said he was fine and he lived 8 more years. also why do we need to spend 3k on a scan when echo works 80% of the time? just saying lol
James Roberts
Oh, so let me get this straight. You’re telling me that a $3,500 machine that takes an hour and requires you to hold your breath while being screamed at by a robot is the ‘gold standard’… while the $1,000 machine that’s done in 20 minutes and lets you chat with the tech about your dog is ‘flawed’?
Look. I get it. MRI sees scar tissue. But how many people actually need to know about fibrosis before they’re symptomatic? Most of us just want to know: ‘Is my heart gonna stop?’
And guess what? Echo tells you that. MRI tells you what kind of scar it is. Which is cool. But if you’re not a cardiologist doing research? You don’t need it. Stop making people feel guilty for not having a ‘gold standard’ scan.
Also-AI echo is getting scarily good. That 4.2% variability? That’s almost MRI-level. We’re not far off.
Marie Crick
This is why we’re losing the war on healthcare costs. MRI is not a ‘deep dive.’ It’s a luxury. Echo is the standard for a reason: it works. If you can’t afford MRI, you’re not ‘missed.’ You’re just getting good care.
And if your doctor recommends MRI because they’re scared of liability? That’s malpractice. Not medicine.
Courtney Hain
Let me guess-this whole post was written by a radiologist who owns an MRI machine. Or maybe a pharma rep pushing gadolinium. Because here’s the real story: MRI is being pushed because it’s profitable. Echo doesn’t make money. MRI does.
And don’t get me started on gadolinium. That stuff stays in your brain. For life. Studies from 2021 show microdeposits in the cerebellum of patients with normal kidney function. No one talks about it.
Meanwhile, echo? No radiation. No toxins. No claustrophobia. Just sound waves. Safe. Simple. Effective.
They’re not ‘complementary.’ They’re being manipulated. Echo is the people’s tool. MRI? It’s a profit center disguised as science.
Jeremy Williams
Having trained in both the U.S. and Japan, I’ve observed that the dichotomy between echo and MRI is often overstated. In Japan, where healthcare is tightly regulated and cost-conscious, 3D echocardiography with strain analysis has become the de facto first-line modality for cardiomyopathy workup. The data is robust. The outcomes are equivalent.
Moreover, the notion that MRI is ‘universally superior’ ignores the fact that in low-resource settings, echo remains the only viable option-and it saves lives daily. Technology should serve equity, not hierarchy.
Ellen Spiers
The author’s assertion that MRI demonstrates superior inter-observer reproducibility is empirically valid; however, the clinical utility of this metric must be contextualized within the framework of evidence-based decision-making. The 2.6% variability in MRI measurements, while statistically significant, rarely alters therapeutic management in routine clinical practice.
Furthermore, the cited 19% discrepancy in wall thickness measurements between echo and MRI is confounded by the use of 2D echo in the referenced study. Modern 3D echocardiographic platforms, when coupled with speckle-tracking analysis, demonstrate concordance with MRI in >90% of cases for LV mass and volume.
Consequently, the rhetorical elevation of MRI as a panacea is both misleading and potentially harmful, as it incentivizes overutilization and exacerbates healthcare inequities. Echo remains the cornerstone of cardiovascular assessment. MRI, while invaluable, is a specialist tool-not a replacement.
Greg Scott
I’m a tech who runs echo machines. We do 20 a day. I’ve seen the same patient twice-once on echo, once on MRI. Echo said ‘normal EF.’ MRI said ‘EF 42% with mid-wall fibrosis.’
We changed his meds. He’s back to hiking.
So yeah. Echo’s great. But don’t ignore the MRI when it’s needed. I’ve seen too many people get told ‘you’re fine’ and then collapse six months later.
Just listen to the patient. If they’re not okay, get the MRI.
Scott Dunne
It is a national disgrace that the United States, with its astronomical healthcare expenditures, continues to underutilize echocardiography as a primary diagnostic modality. In Ireland, we have universal access to high-end echo. No waiting. No cost barriers. We do not chase MRI like some kind of holy grail. We trust the clinician. We trust the sound waves.
This post reads like a corporate marketing brochure for GE Healthcare. Echo is not ‘flawed.’ It is underappreciated. And the obsession with MRI is a symptom of American medical overconsumption.
Ashley Paashuis
One of my patients had recurrent unexplained syncope. Echo was normal. MRI revealed a small fibrotic patch in the right ventricle-later confirmed as arrhythmogenic cardiomyopathy. She’s now on an ICD and hasn’t had another episode.
But here’s what I want to say: we don’t need to pit these tools against each other. The real innovation isn’t choosing one over the other. It’s integrating them. Imagine a clinic where echo is done in the morning, and MRI is scheduled for the afternoon-both interpreted together by a team. That’s the future.
And yes, we need to fix access. No one should wait 3 weeks for a scan just because they’re not rich.